The title of this paper references five terms of specific importance to my understanding of global health humanities, as the subfield has emerged since the latter part of the twentieth century. The first and second terms—global health and comparative literature—juxtapose two domains of knowledge often held apart disciplinarily: in other words, they are considered two modern disciplines often thought of as methodologically, and even incommensurably, distinct. And they are held apart with a continual insistence on the differences in their perspectives or fields of vision, their modes of analytical work, and their approaches to human existence as manifested in cultures of art and medicine. The fourth and fifth terms—HIV and South Africa—are now, since Thabo Mbeki’s brand of denialism has become less potently pervasive, frequently associated in the literature on global health and sub-Saharan Africa. These terms carry with them a set of medical and geopolitical connotations, and they are made to overlap as they represent a set of infected and nationalizing bodies, as they co- inhabit disease and geopolitical imaginaries for what in the past we might have called the third or developing world, and currently call the global south or regions of low-resource communities. It is my intention to further discuss the first two and last two terms, rather conventionally I must admit, as this essay progresses. But it is in my use of the third term (perspective), as an aspect of literary analysis and form, that I hope my argument will coalesce.
To de-provincialize health from the clinical, natural, and social sciences is to open a space for broader comparative undertakings. . . it is to increase the capacity of the epistemological imagination to pose questions about how literature and medicine help us know what we know about the World and Africa, as well as what that knowledge is grounded upon.
For what I wish to do in the space I have is illustrate one place that comparative literature—and by this I mean literature in different cultural or disciplinary languages as well as literary study across those languages—may hold in ethics deliberations concerning the field and practice of global health and world literature. The examples will undoubtedly draw from my current status as a faculty member anchored in two departments: that of comparative literature and internal medicine. But they will also derive from having spent some time researching the place of literature in health care settings in Africa and also teaching its attendant place in courses dedicated to bioethics. These examples help advance an argument with three broad claims.
First, I argue that working in fields of expansive geopolitical scale, and in fields conceived via notions of human and ecological difference (e.g., tropical medicine, global health, African literature, world literature), requires specific processes of the imagination that are often naturalized or rendered invisible to specialists in these fields, but are most evident and best examined in genres of openly imaginative literature. Second, I argue that literary narrative forms, like the novel and memoir, have served as alternative sites of ethical inquiry, especially for acts of care or culture that take the world as its starting point or primary frame, for acts that understand from the beginning that most members within its communities of care or culture will never meet or know one another beyond what the imagination makes possible. And third, I argue that the mode of ethics analysis made possible by creative uses of the imagination is important for revising standards of thought and practice for these acts of care and culture. It is a mode of ethics rarely emphasized in professional genres of health and legal practice, philosophy, or policy. It also represents a significant absence since ethics, I insist, is crucial for maintaining a distinction between our current work in global health and world literature and the work of our colonial counterparts during the late-nineteenth to mid-twentieth century.
Put differently, I argue that present-day versions of global health and world literature have a central problem. Yes, contemporary specialists are especially attuned to the colonial legacies, histories of underdevelopment, and processes of disenfranchisement that have produced inequalities in the distribution of health and literature, inequalities that we (as practitioners and scholars) seek to address. Yet many of us find it difficult to rigorously distance our current work from the work done by our colonial predecessors. This remains the case even though we repeatedly rename our fields: the adjective before medicine has periodically shifted from missionary medicine to colonial, tropical, international, world, and now global health. While the adjective before literature has also periodically shifted, from world literature in the nineteenth century to, much later, commonwealth, third-world, postcolonial, world again, and even global/Anglophone. It is not always certain that these shifts in denotation have ensured shifts in connotation (for example a breast cancer specialist for patients in Menlo Park may be doing medicine, as opposed to a malaria specialist in Britain travelling frequently to Uganda; we can think of equivalents for writers of fiction or memoir). And this uncertainty feels all the more certain as one notices present-day versions of these fields gather specialists who continue to be concerned with and for foreign others, who continue to work across similar if not the same national borders, and with similarly expansive geopolitical scales in mind.
In fact, I’d say that the distinction between present-day global health and world literature and earlier, colonial forms of these fields is not convincingly made when we say any of the following:
- that we should pay fuller attention to the plight and literary accounts of others (if you look through medical journals of the nineteenth century, like The Lancet, and the writings of missionaries, you will see numerous examples of this same call)
- that we should sympathize more fully with the health plight of others abroad and elicit that fuller sympathy via the sending and receiving of cultural objects, narratives, and images of suffering (there is, in fact, a long tradition of these attempts in journals, the writings of physicians like Albert Schweitzer, and novels from the nineteenth century on)
- that we should more fully address the health plight and account of others abroad by enhanced techniques of interpretation, diagnosis, and delivery, in the realms of science, medicine, and literature (actually, tropical medicine was founded on the promise to use and export the best current interpretative and diagnostic technology, the microscope, and there were similar goals articulated during early and mid-twentieth-century eradication programs; this is also a recurring refrain for the translation, interpretation, and distribution of foreign accounts, from the travel writing and world literature of the nineteenth century on)
- and that we should understand the health plights and creative accounts of others abroad to have consequences for those of us living at home, within the increasingly porous borders of a nation-state (this is pretty much the essential presumption of modernist fiction at the turn of the twentieth century, by Conrad, Gide, Woolf, and a similar understanding gave health some space in the Covenant of the League of Nations in 1919, as it developed an argument for international medicine that was inseparable from that for international security, economics, and peace).[1]
I would say, though, that those of us concerned with problems in global health and world literature do begin to successfully distinguish our work from earlier colonial forms in the specific ways we examine the ethics of what we do. In other words, I argue that current developments in ethics—as a field with robust conversations at intersections with literature as well as medicine—can constitute a point of demarcation between colonial and present-day versions of what we do. And as someone housed in departments of comparative literature and medicine, my work is animated by ways to have these two, often separated ethics conversations collaborate in making the distinction from our colonial predecessors rigorous and sustained.
Over the course of this essay, I will focus on the issue of delivery: as a perennial concern for the field of global health and those working through problems of health care delivery in low-resource communities abroad, and as a perennial concern for the field of comparative and world literature and those working through the problems of reading the novel as a means for delivering others across cultures and axes of inequality.
For a set of clarifying examples, I will present three pairings of theoretical, medical, and literary writings on the subject. The first is a pair of insights about delivery in global settings: one offered by Paul Farmer, a professor of global health, in his 2013 Shattuck lecture, titled "Chronic Infectious Disease and the Future of Health Care Delivery;" and another by David Palumbo-Liu, a professor of comparative literature, in his 2012 book, Reading Literature in a Global Age: the Deliverance of Others.
The second pairing is drawn from the mid-twentieth century. I will place the preamble of the Constitution of the World Health Organization (WHO), drafted and published in 1946 next to a pivotal scene in Albert Camus’ novel, The Plague, drafted during the same period and published in 1947.
And the third pairing is drawn from two early-twentieth-century narratives of HIV delivery in South Africa. I will pair passages from Jonny Steinberg’s (2007) Sizwe’s Test, a journalistic account of a young man’s relationship to testing and treatment, and Kgebetli Moele’s (2009) The Book of the Dead, a novel of communal infection partly narrated by the virus itself as it describes moments of its own transmission from member to member of a South African society marked by the disease.
Lastly, it is important to say here that these pairings are elaborated upon within the context of a book project I am developing, titled Forms of Global Health, where I study the place of literature in the development of past and present fields of transnational medicine, comparing the influence of long narrative forms during the emergence of tropical medicine as a colonial endeavor at the turn of the twentieth century with the emergence of a literature of global health, especially the novel, at the turn of the twenty-first.
The broader stakes of my argument there is that studying literary discourses in the disciplinary settings of transnational medicine is of importance to contemporary fields of African, world, and comparative literature—primarily because comparative literature has been especially attuned to the literary epistemologies and the literary ethics of projects that take the world as an organizing rubric. Such scholarship has been done in the world’s varied languages. It has at once honed and opened up notions of literature as they clarify in distinct though interconnected contexts. And yet I argue that scholarship in comparative and African literature will by definition remain incomplete—will continue to contain within it a version of Achille Mbembe and Sarah Nuttall’s (2004) "epistemological abyss"—without attention to how literature has served as a discursive source for projects of transnational health during colonial and postcolonial periods and as a means for writers and readers to examine the ethical implications of those projects. If I were to continue to paraphrase or essentially rewrite a passage from Mbembe and Nuttall’s (2004) essay, "Writing the World from an African Metropolis," I would reassert the stakes of my project as follows: that to de-provincialize health from the clinical, natural, and social sciences is to open a space for broader comparative undertakings. It is to increase the capacity of the epistemological imagination to pose questions about how literature and medicine help us know what we know about the World and Africa, as well as what that knowledge is grounded upon.
A Shared Focus on Delivery
In his 2013 Shattuck Lecture, reprinted in a special issue of the New England Journal of Medicine on "Failures of Delivery," Paul Farmer defines the recurring problem of global health to be the difficulty of addressing the delivery gap: where decreasing mortality and morbidity rates have lead to an increasing burden of chronic diseases, for which we now have effective therapies, but inadequate innovation for delivering them efficiently to the neediest people. Farmer is worth quoting here at length:
As compared with discovery science and randomized trials, the 20th-century biomedical paradigm viewed care delivery as scientifically uninteresting—too messy for serious scrutiny, like the observational and qualitative methods that elucidate it. Yet understanding how and why care delivery does or does not happen and how to improve it may now represent medicine’s most important task. (Farmer 2013. 2424)
For those who know Farmer’s writings, this passage is very much part and parcel of an ongoing effort to "re-socialize medicine," which is to bring the social sciences to bear on health care practice and scholarship in deeply transformative ways. This is why you see in this passage several allusions to modes of analysis: discovery science, randomized trials, serious scrutiny, observational and qualitative methods that are too messy, but do, he argues, elucidate. What they elucidate is not simply what was or was not delivered, but the how and why of the delivery gap, two sets of questions that many practitioners and scholars seek to answer under the contemporary ethics rubric of distributive justice. I would like to point out that the specific hows and whys that Farmer goes on to address in this and other lectures are precisely those very capably answered via the social sciences. But for anyone like myself, who both understands the effort to re-socialize medicine and yet wishes to respond to the perennial call to re-humanize health, Farmer’s lectures continue to provoke questions concerned with regarding method, particularly the ways literature could make clear a different set of hows and whys of substandard delivery in transnational settings.
One very important starting point can be found in David Palumbo-Liu’s study of world literature as a system for delivering characters to readers and imaginary others to a global audience. Here I quote:
how is it, today, that we can best understand the nature of how the other is delivered to us, and we to "them," and how does literary narrative offer a particular mode of deliverance, of imagining the affective connections among others, different from the delivery systems we have investigated and their assumptions of human sameness? Most specifically, how can literary texts capture the phenomenon of system overload—how can we imagine otherness outside and beyond the "delivery systems" that run on common units. What kind of alternative critical delivery system might literature be? (Palumbo-Liu 2012,142)
There is much in this paragraph, but I’d like to focus on the questions Palumbo-Liu raises about two sets of methods: first, how novels may function as alternative and critical, even ethical delivery systems, and second how we may be able to read and understand novels as doing that ethical work. Answering these questions in the setting of medicine has led me to consider novels to be sites of highly prescient ethical inquiry—able to utilize systems of the imagination to think past the methodological boundaries often set by other genres of writing. In the specific instance of medical experimentation on vulnerable populations we have as an enduring example Mary Shelley’s Frankenstein (1818), but also Toni Morrison’s Beloved (1987), Rebecca Skloot’s Immortal Life of Henrietta Lacks (2010), and Kazuo Ishiguro’s Never Let Me Go (2005). In the specific instance of global health, I would like to offer Albert Camus’ novel, The Plague, precisely because it was conceived and published in 1947, alongside the 1946 constitution of the WHO, and so presents itself as a striking example of the alternate mode of ethics deliberation made possible by a turn to the novel, after WWII, during a period of heightened awareness of the repeated dangers of nationalism and the need to reimagine a world community and to develop rationales for caring for that community with not only imaginable dimensions and membership, but also for working across and beyond various sets of recognized borders.
Many (including Paul Farmer) consider the WHO to be the first global health institution. Part of the reason for that is the scale of its Constitutional Preamble, and the articulation of precepts for health that continue to be repeated and revised through the twentieth and now twenty-first centuries:
THE STATES parties to this Constitution declare, in conformity with the Charter of the United Nations, that the following principles are basic to the happiness, harmonious relations and security of all peoples:
- Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.
- The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, and political belief, economic or social condition. The health of all peoples is fundamental to the attainment of peace and security and is dependent upon the fullest cooperation of individuals and States.
- The achievement of any State in the promotion and protection of health is of value to all.
- Unequal development in different countries in the promotion of health and control of disease, especially communicable disease, is a common danger.
- Healthy development of the child is of basic importance; the ability to live harmoniously in a changing total environment is essential to such development.
This last article provides a focused point of comparison with a well-known scene in Camus’ novel that is set in a town, Oran, in a nearly deracinated Algeria, during a plague epidemic, where a boy is given an experimental drug and observed by several adults, who make up an emergency public health team:
The doctor’s hands were gripping the rail of the bed, his eyes fixed on the small tortured body. Suddenly it stiffened, and seemed to give a little at the waist, as slowly the arms and legs spread out X-wise. From the body, naked under an army blanket, rose a smell of damp wool and stale sweat. The boy had gritted his teeth again. Then very gradually he relaxed, bringing his arms and legs back toward the center of the bed, still without speaking or opening his eyes, and his breathing seemed to quicken. Rieux looked at Tarrou, who hastily lowered his eyes.
They had already seen children die—for many months now death had shown no favoritism—but they had never yet watched a child’s agony minute by minute, as they had now been doing since daybreak. Needless to say, the pain inflicted on these innocent victims had always seemed to them to be what in fact it was: an abominable thing. But hitherto they had felt its abomination in, so to speak, an abstract way; they had never had to witness over so long a period the death-throes of an innocent child….
[Later a character asks the presiding physician] "Will you have to start it all over again? [meaning the experiment with the drug; the doctor responds]
"Perhaps. After all, he put up a surprisingly long resistance."
[And, a few paragraphs later, a presiding religious father says to another doctor] "Why was there that anger in your voice just now? What we’d been seeing was as unbearable to me as it was to you."
"I know I’m sorry…"
"I understand," the father says, "That sort of thing is revolting because it passes our human understanding. But perhaps we should love what we cannot understand."
"No Father. I’ve a very different idea of love. And until my dying day I shall refuse to love a scheme of things in which children are put to torture." (Camus 1947, 214–218)
I’d like us to first simply note how Camus’ novel encourages a different mode of ethical thinking in the past and in the present. In the 1940s the novel—as in this one scene—is able to open up and examine several words, terms, and notions being developed as declarations of health in the WHO’s constitution. But I’d also like us to contemplate what this scene of a dying child continues to deliver to readers of Camus’ novel in the present. Let us just focus on the last line—and keep in mind recent events concerning the Ebola epidemic—then ask the following: what would be the ethical significance of us reading a physician’s declaration that "until my dying day I shall refuse to love a scheme of things in which children are put to torture"? What scheme would he be refusing to love? Scheme here could certainly refer to the medical experimentation that may have prolonged suffering, to God’s Will in the form of a seemingly unwarranted plague or epidemic (see conversation with the father); it could also refer to the order and will of nature (the natural history of epidemic as a genre), the repetitive rise and excess of nationalism (Camus is of course thinking of WWII and Nazi Germany), the troubled intensification of colonialism (it is set in Algeria) and the processes of underdevelopment that will continue to unfold in that country and its commonwealth of postcolonial states. But scheme could also read as the international and world apparatuses that in their articulation of health may continue to place emphasis on treatment over prevention, on emergency response to medical and security crises over the sustained and gradual development of infrastructures of care. Scheme here could read for us as the repeating plots and settings of outbreak narratives, with their attendant imagery that call for periodic and disruptive action. See for example, the discourses of outbreak in sub-Saharan Africa, continually framed by images of Biafra, producing a genre of call-and-response that has been naturalized to the point of intertextual composition in the case of Ethiopia and pseudo-voyeurism in the case of Sudan. Right through to the Ebola crisis of 2014–15, where a recurrence of child-associated images comes to frame a now established subgenre of global health discourse. Like that of Cynthia in Monrovia and Sophie Doe and her grandchildren.
Images That Deliver
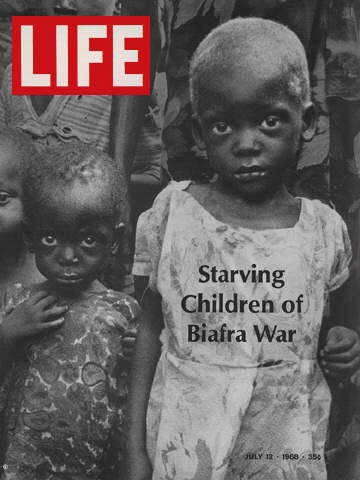
Life Magazine cover, July 12, 1968.
![]()
[ Click icon to see photo ] The photojournalist Raymond Depardon filming a child suffering from famine during the Biafra war in July, 1968 in Nigeria. (Photo by Fondation Gilles CARON/Gamma-Rapho via Getty Images)
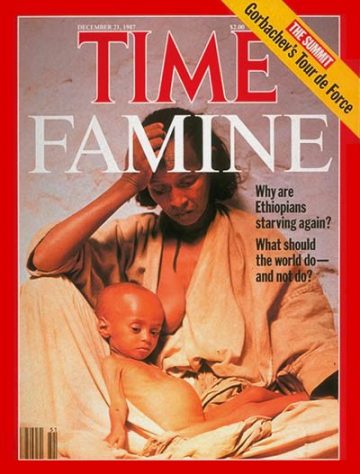
Time Magazine cover, December 21, 1987. (Photo by William Campbell)
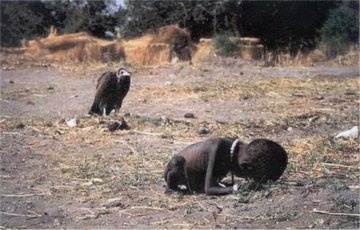
Vulture watching a starving child in Sudan, 1993. (Photo by Kevin Carter/Sygma Corbis – low res image from Wikimedia commons)
![]()
[ Click icon to see photo ] A sick child that health workers called Cynthia, lay on the a concrete rise as waited for Liberian Health workers to remove dead bodies before she could enter the Redemption Hospital in the neighborhood of Monrovia that locals call ‘New Kru Town on Saturday September 13, 2014 in Monrovia, Liberia. (Photo by Michel du Cille/The Washington Post via Getty Images)
![]()
[ Click icon to see photo ] Sophia Doe sits with her grandchildren Beauty Mandi, 9 months (L) and Arthuneh Qunoh, 9, (R), while watching the arrival an Ebola burial team to take away the body of her daughter Mekie Nagbe, 28, for cremation on October 10, 2014 in Monrovia, Liberia. The children seen in the photo are daughters of the deceased. (Photo by John Moore/Getty Images)
Delivery/Deliverance via Literary Text
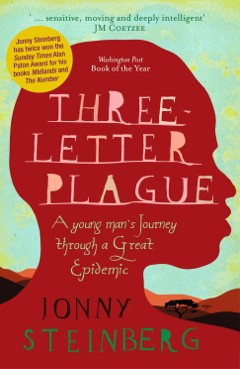
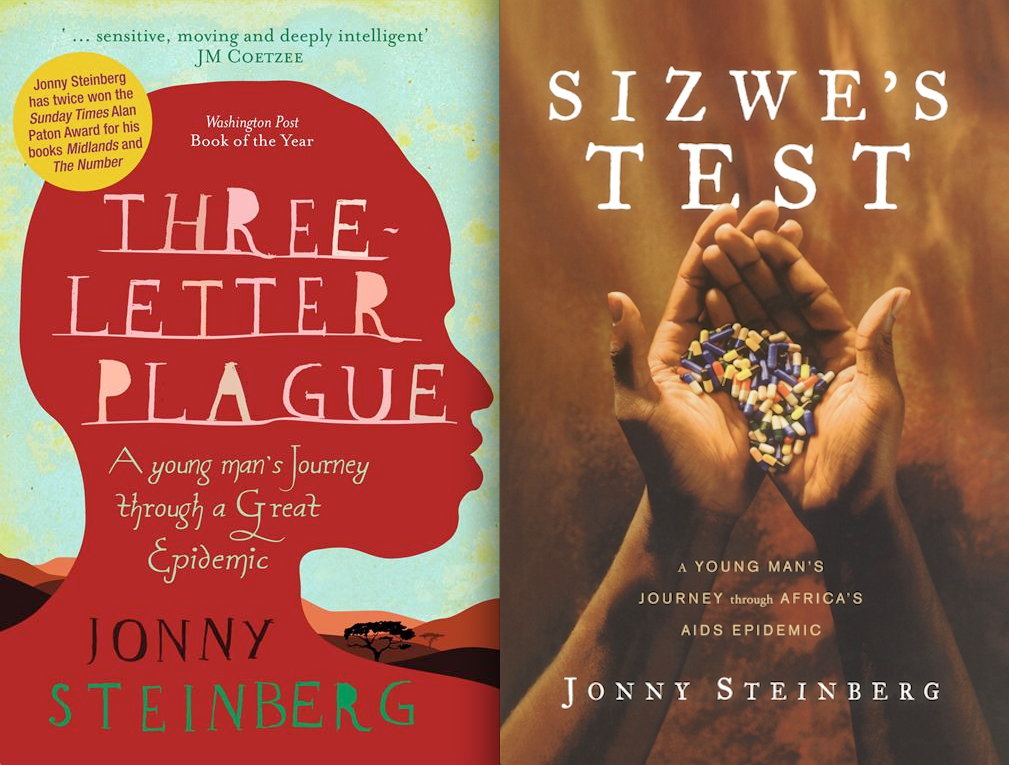
I use images as segue here, because as you can see in just these few, such images very easily delineate a history of delivering others via cultural objects as part of transnational health practice in and for Africa. And that practice, of course, extends to the covers of books about the continent’s pandemics. For example, one should compare the original South African edition for Jonny Steinberg’s book with that of the American edition. Notice, among many things, the shift in central image—from the silhouette of a young man to his hands holding what in the book are called "magic pills." Note, too, that the pills are gathered in the form of the continent. This is accompanied by a change in title and subtitle, from Three Letter Plauge to Sizwe’s Test: A Young Man’s Journey Through a Great Epidemic to Sizwe’s Test: A Young Man’s Journey through Africa’s AIDS Epidemic.
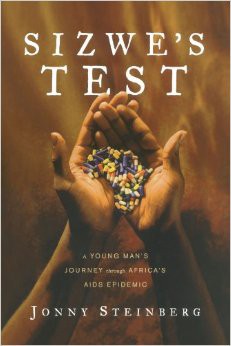
Now, Steinberg’s book is a work of very perceptive literary journalism about a doctor’s hard work in a local community with a significant though not fully measurable incidence of HIV, where he tries to get men like Sizwe to come for testing and, if infected, into steady treatment. But the framing of the US cover delivers the account as immersive reporting from the frontlines. So, I argue, Sizwe’s Test/Three-Letter-Plague struggles to be read fully. If we do read it fully, we find that it isn’t really (or simply) an account of a journey, as the subtitle suggests, or a new form of travel writing (for us to receive). It is instead a questioning, a repeat articulation of the how and why of a specific gap in delivery. Even the author himself becomes surprised by the importance of questions. Near the end:
On the day of our telephone conversation, some 262,000 people have begun antiretroviral treatment at public health-care facilities in South Africa. More than two-thirds of them are women. Why? Where are the missing men? Why are they so less likely to find their way to ARV treatment than women? That is not the question I set out to answer when I began writing this book, but it has been hard not to notice it on every page. (Steinberg 2008, 325)
I would argue that—via his writing—Steinberg has found himself to be within the delivery gap Paul Farmer defined for us earlier, at the limit of what strict journalism can record, what any form of ethnography can observe or explain, at the limit, too, of what the clinical and social sciences can do, and so he is compelled to pay closer attention to the page, as itself a mode of understanding how standards of care come to be. It is no mistake, I argue, that this resembles a literary form of ethical attention. So I return here to David Palumbo-Liu’s question: "What kind of alternative critical delivery system might literature be?"
An illuminating example can be found in Moele’s novel The Book of the Dead, where he takes us to scenes narrated from the perspective of HIV. What I’ll quote below is between a boy (Thapelo, aka little gangster) and his father (Khutso), with HIV narrating from inside Khutso, so that "I" has a double register:
"I am terrified of Aids. I hate Aids, Dad, I hate it," the little gangster continued. "If Aids were a person, I would kill him or her with my bare hands, but there is no Aids, there are only people, and that is the worst thing about Aids." True, there is no Aids, only people, I thought, listening attentively. "Do you know how many suicides we have had at school this year?" he asked me, knowing full well that I had no idea. "Four. And that was after a girl who was sleeping around died an Hiv-related death. . . ."
"Thapelo, you just keep on abstaining," Khutso told the little gangster, even though he hurt me by saying it. "But I can’t abstain for the rest of my life, can I?" Thapelo said. "No, I can’t, and that is the worst thing, because once I take off my under-wear it’s like putting my head in a hangman’s noose and waiting for the ground to give way beneath my feet, all the time hoping that it doesn’t. I don’t trust my girlfriends, but I am a hypocrite because I have three of them. . . . I am also untrustworthy. And once I start sleeping with them, I will be putting my head in the hangman’s noose, and one day the ground will surely give way and I will hang. There is no way around it, Dad. Or is there?" He looked at me, hoping that I would be able to give him some kind of an answer, but Khutso had nothing to say. I smiled. I am coming for you, little gangster, I thought quietly to myself. You are right, there is no way around it." (Moele 2009, 163-164)
For the space I have here, there is simply too much to work through in this one passage. I ask us to notice just that the last few lines are in the voice of the virus that has occupied Khutso (the father). And so when you read back up from the end you move from HIV smiling at the present scene, watching a father have nothing to say to his son, who asks un-innocent much-too-mature questions that one can’t help but notice on the page. If Steinberg seems to ask a sociological or anthropological question about the delivery gap—where are the men?—we ought to pay attention to how Moele, the novelist, begins to answer it literarily. The men, in essence, are here: in this kind of scene where HIV and father are one, unable to help a son answer the pressing questions of a chronic epidemic, and only able to watch, as HIV does, as the boy enters the scene-to-come suggested at the end of the passage.
Conclusion
I have made several allusions to the Ebola epidemic, and in closing I’d like to return to David Palumbo-Liu’s question: "What kind of alternative critical delivery system might literature be?" There is a sense of the future tense in that question, not just for future ways in which we may read and incorporate novels in our ethics work, but also for ways in which we may rewrite the genres we work with and participate in. Note, therefore, that in Paul Farmer’s latest comment on Ebola, titled "Diary," and published in The London Review of Books, that there is a tone of world weariness in his account and repetition of sociological explanations for the epidemic:
Ebola is more a symptom of a weak health care system than anything else. But until this diagnosis is agreed on, there’s plenty of room for other, more exotic explanations. . . . The palaver (as Liberians say) includes a lot of talk about the "cultural beliefs and behaviours" said to propagate the outbreak. The list usually includes activities that are not really "behaviours," such as hunting and eating bush meat, taking part in strange funerary practices or the bizarre rituals of "secret societies" like the Poro or the Human Leopard Societies. An obsession with funerary rituals—the more lurid the better—was characteristic of anthropology from the late 19th century on. Tribes of the Liberian Hinterland (1947), written in the passive voice and matter-of-fact tone typical of the genre, contains more than five hundred pages of this sort of stuff…. Less palaver, more action. (Farmer 2014)
What Farmer seems to be offering here is a messy, unclassifiable though rigorous explication of patterns of representation and the senses of responsibility they produce. He seems to be on the verge of refusing to write in an expected way. And as specialists in global matters, we might be able to think of him heeding the refus of Camus’ novel, starting to imagine himself as a physician-character refusing to love a scheme that expects him to respond, to participate as hero in a particular kind of novel, account, or genre for global health. Again made accessible to us as the diary of a physician and anthropologist, published in The London Review of Books. In one sense, he offers what we could begin to call a narrative ethics for global health.
Notes
References
Camus, Albert.1947. The Plague. Translated by Stuart Gilbert. New York: Vintage Books.
Farmer, Paul. 2013. "Chronic Infectious Disease and the Future of Health Care Delivery." New England Journal of Medicine 369 (25): 2424–2436.
——— 2014. “Diary.” London Review of Books 36(20): 38–39, http://www.lrb.co.uk/v36/n20/paul-farmer/diary.
Jameson, Fredric. 1990. "Modernism and Imperialism." In Nationalism, Colonialism, and Literature, pp. 43-66.. Minneapolis: University of Minnesota Press.
Mbembe, Achille, and Sarah Nuttall. 2004. "Writing the World from an African Metropolis." Public Culture 16 (3): 347–372.
Moele, Kgebetli. 2009. The Book of the Dead. Cape Town: Kwela Books.
Palumbo-Liu. David. 2012. Reading Literature in a Global Age: The Deliverance of Others. Durham, NC: Duke University Press.
Said, Edward. 1994. "A Note on Modernism." In Culture and Imperialism, pp. 186–190. New York: Vintage Books.
Steinberg, Jonny. 2009. Sizwe’s Test: A Young Man’s Journey Through Africa’s AIDS Epidemic. New York: Simon Schuster.
Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License

{kind=link}